

Ectodermal dysplasia can present with a variety of manifestations. 1/10,000 people are affected in different ways. Patients can show up with signs of sparse hair, malformed sweat glands, abnormally developing nails, skin diseases, vision disturbances, hypo or anodontia. Considering that this is a hereditary condition present at birth, the psychosocial effects on the patient are incredible.
When it comes to hypo or anodontia, without early interceptive treatment the patient is set up for a life of psychological, developmental and functional distress. With malformed alveolar ridges, or missing/misshaped teeth – mastication, speech, muscular functions, esthetics and socialization are all compromised.
We now present a case of the youngest recorded patient to receive dental implants as a result of ectodermal dysplasia.
Case Presentation
A 3-year-old girl presented with her parents with a chief concern of the child’s malformed and partially missing primary teeth. The child showed several signs of ectodermal dysplasia: hypodontia, sparse hair, hypohydrosis, dermatitis. She also has a bilateral cleft lip and palate that was surgically repaired at 6 months of age. She was diagnosed with Hay-Well syndrome, just like her father.
Clinical and radiographic examination showed multiple missing teeth and a few developing tooth buds.
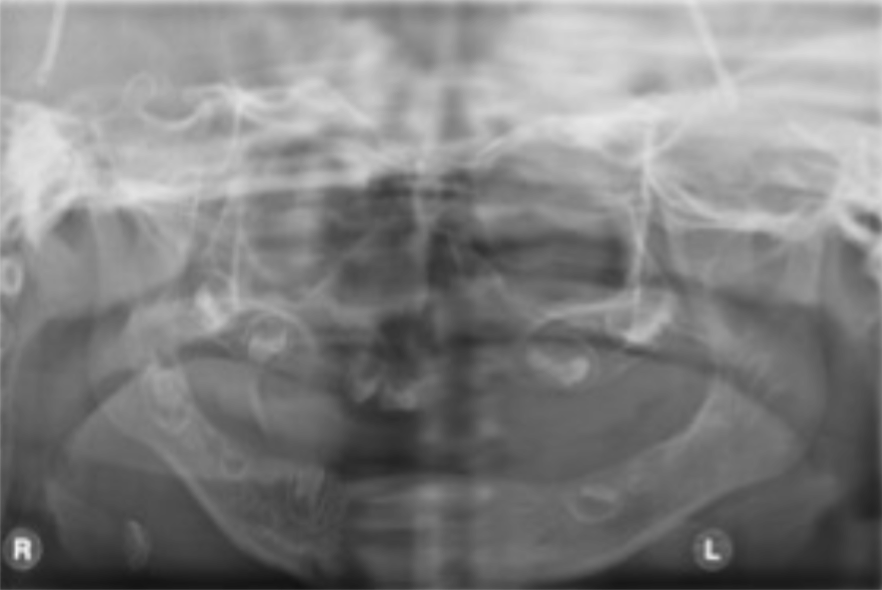
It was first decided to wait for further growth to determine the extent of her oral manifestations of the disease. However, at 5 years old she had all of her primary teeth extracted, as they were severely malformed with poor prognosis. Upper and lower complete dentures were made, but understandably she could not wear them due to limited sulcus depth and lack of retention from restricted lips and palatal cleft defect.
Collaborations between pediatric dentistry, oral surgery, and restorative dentistry lead to treating the patient with maxillary implant supported overdentures. Implant were not a viable option in the mandible as per insufficient bone.
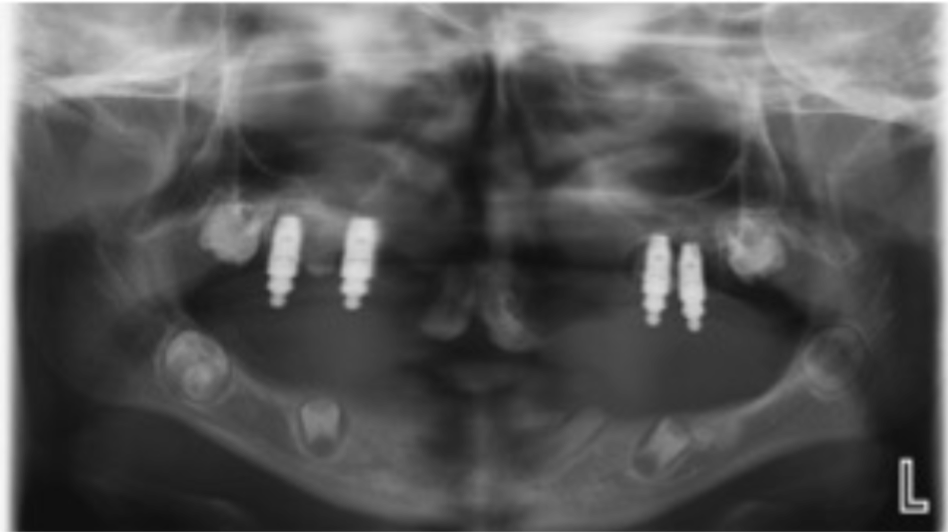
At 6 years old, 2 implants were placed in the canine region and 2 in the premolar region of the maxilla. The implants were restored with ball attachments and overdentures 6 months later. The lining of the overdenture was a silicone material, in order to absorb mastication forces, allowing for patient facial development, and to close the residual cleft palate.

By age 12, implants were placed in the anterior mandible with the fabrication of a lower overdenture. The maxillary overdenture was also replaced as it become less retentive with facial growth. The parents were informed that the overdentures had to be constantly replaced until facial growth had finished. Also, as the patient grew and the gingiva around the implant abutments thickened, the abutment height decreased. Therefore new overdentures with new ball attachments were needed.

| This early interceptive treatment allowed for improved function and nutrition, that would not exist with tissue supported dentures or no intervention at all. This treatment supported the improved development of masticatory and perioral muscles, and the growth of basal bones. The improvements to esthetics, speech and a normalized life can’t be overlooked. Implant placement in children is not well understood. From the few reported cases, the procedure is known to be predictable, with a 5 – 7% failure rate. As the facial structures grow, there is a risk of implant failure or dislocation. Also, as the alveolar bone grows in height, there is a risk that the implants will be submerged. The ideal time for implant placement is when facial growth is completed, but as in the case presented, early treatment is sometimes needed to prevent the harms of no treatment at all. Informed consent and close monitoring is critical for treatment success. |
| This case was completed and reported by Dr. Lisa Clarke (pediatric dentistry), Dr. Louise Bowyer (Oral Surgery), Dr. Jennifer Noone (Pediatric dentistry). |