

Case Presentation
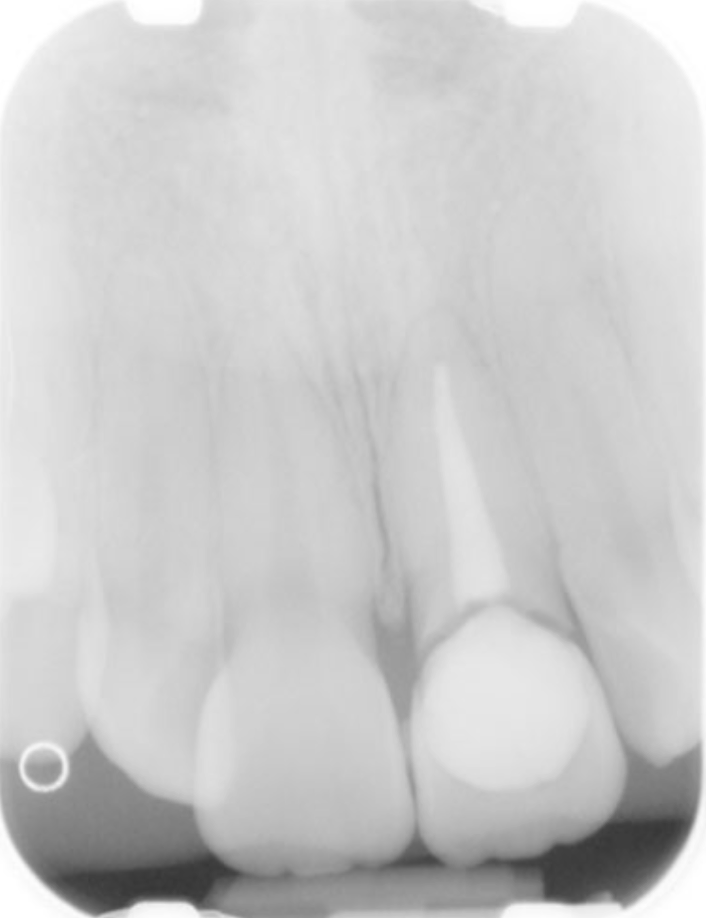
A 19-year-old woman was referred to the clinic with acute pain on the upper left central incisor, as she experienced a sports injury the day prior. The patient had fractured the coronal aspect the tooth. Periapical radiographs showed previous root canal treatment and no signs of root fractures. The upper right central and left lateral incisors responded normally to pulp testing.
The fracture line was just below the free gingival margin on both the buccal and lingual sides, presenting with mobility and tenderness on surrounding periodontal tissues. It was obvious that the coronal fragment was being held in place with gingival fibers.


Urgent Treatment
To provide immediate comfort and relative esthetics, the coronal section of the central incisor was splinted to each adjacent tooth with an orthodontic wire. Post-operative instructions were given to the patient to prevent further damage until definitive treatment could be completed.

Definitive Treatment
2 weeks following the initial visit, the patient presented with an improved soft tissue profile. After discussing all treatment options, it was decided that the coronal aspect of the tooth would be re-attached with a post and core system as an intra-canal anchor.
A silicone index was made using polyvinylsiloxane for reliable repositioning of the coronal fragment.
Following anesthesia and removal of the splint, a buccal and lingual flap was raised to determine the extent of the fracture. As the fracture line did not violate the biological width, osseous crown lengthening would not be needed.


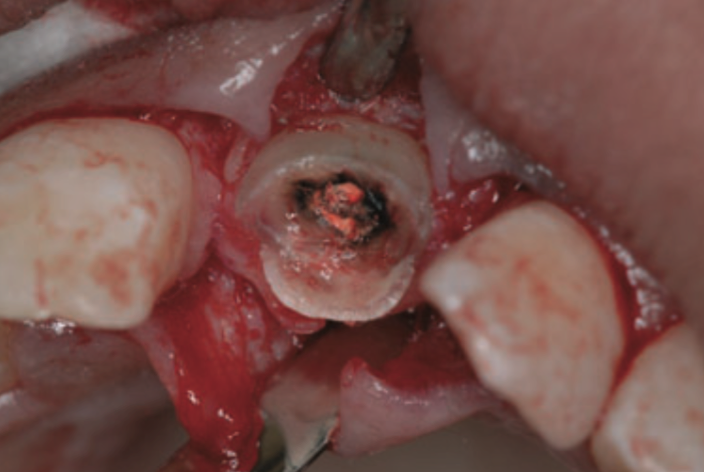
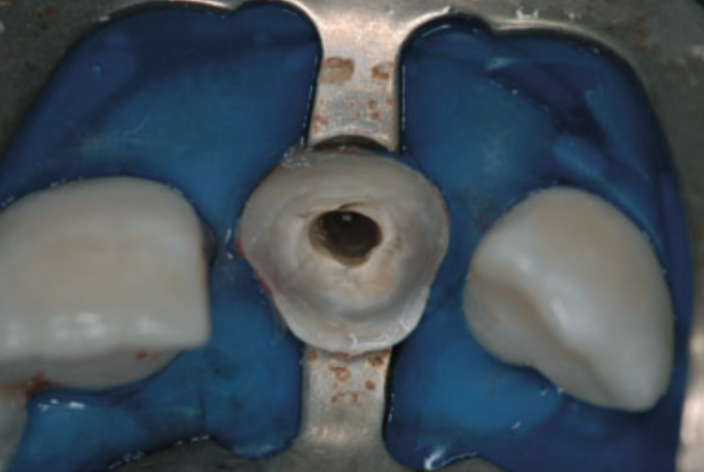
The root length was measured with a periapical radiograph; the root canal was prepared for a prefabricated fiber post (Light Post Illusion #2, Bisco). After cementation of the post, the coronal aspect of the tooth was prepared with the same post drill as was used for root canal, etched, primed and coated with adhesive bonding (Single Bond 3M ESPE). Dual curing flowable resin composite was placed on the lingual aspect of the fractured coronal portion and the cervical of the remaining root. Using the silicone index, the fragment was repositioned onto the post.
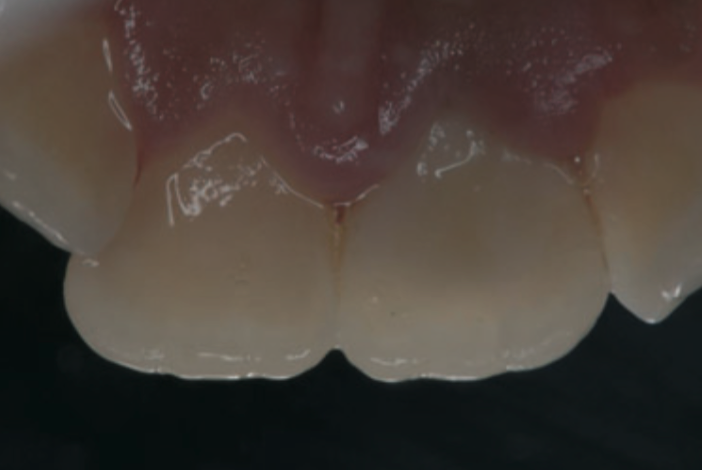
Excess resin was cleaned and the tooth was polished. Two papillary sutures were placed to close the raised flap.



The patient was observed 2 weeks after the procedure and presented with tooth asymptomatic and no discomfort. The patient was followed up for 4 years, were the tooth was still holding on strong.


| Whenever a patient presents with a complicated fracture of an anterior tooth, many options are available. Initially, we can extract the tooth and prepare for a single implant placement. We can also theoretically plan for post/core build-up and crown placement, while achieving adequate ferrule with crown lengthening or orthodontic extrusion. However, orthodontic extrusion would result in a cervical discrepancy between the central incisors. The procedure presented shows the most conservative treatment option for a fracture of this extent. In case this treatment fails, we still have all other options available. Furthermore, this treatment option instantly regains esthetics and function for the patient, compared to the other treatments discussed that can take months. |
| This case was completed and reported by Dr. Gustavo M. S. Oliveira, Dr. Greice B Oliveira, Dr. Andre ́ V. Ritter. |