
")
Dealing with dental fluorosis is tricky. Depending on the severity of the hypomineralization, there are many different treatment options. Sometimes the issue is solved with simple bleaching, yet sometimes veneers/ or crowns are needed to mask the unappealing “white spots.” Unfortunately, many times the treatment of choice presents itself through trial and error, after exhausting all less invasive treatment options.
Dental fluorosis is caused by hypomineralization due to the effects of excessive fluoride on ameloblasts during enamel formation – resulting in surface pores. This usually happens when the patient is around 15 to 30 months. Although hypomineralization doesn’t cause any functional issues, its main consequence is compromised esthetics. And when dealing with adolescent patients, compromised esthetics can have profound psychosocial effects.
A new material that was originally manufactured for caries infiltration has shown promising results when used to treat fluorosis spots. Low viscosity light-curing resins can rapidly penetrate the micro-porosities of fluorosis lesions. After etching the lesion with hydrochloric acid gel, the resin can be applied. The resin is penetrated into the lesion body by capillary forces, and by being able to dictate the shade of the resin, we can blend the micro-porous areas to the rest of the tooth.
This new material allows us to solve such a crucial problem, without having to reduce tooth structure in repeated bleaching or crown/veneer preparations.
Treatment Protocol
- After the teeth are isolated, they should be cleaned with prophylaxis paste and treated with 15% hydrochloric acid gel for 120 seconds. The entire surface of the tooth should be etched to achieve a homogenous surface. Following 120 seconds of application, the etch should be washed with water for 30 seconds. This etching procedure removes the more mineralized superficial layer of the enamel to allow for better resin penetration.
- To remove the water retained in the micro-porosities, the surface of the teeth should now be treated with ethanol for 30 seconds and air-dried.
- The flowable resin (Icon- infiltrant) can now be applied to the teeth. The excess should be wiped away with cotton rolls and light cured for 40 seconds. This application of resin can be repeated more than once to achieve more profound results and to further minimize enamel porosity.
- Finally, the roughened enamel surface can now be polished with your favorite composite polishing disks.

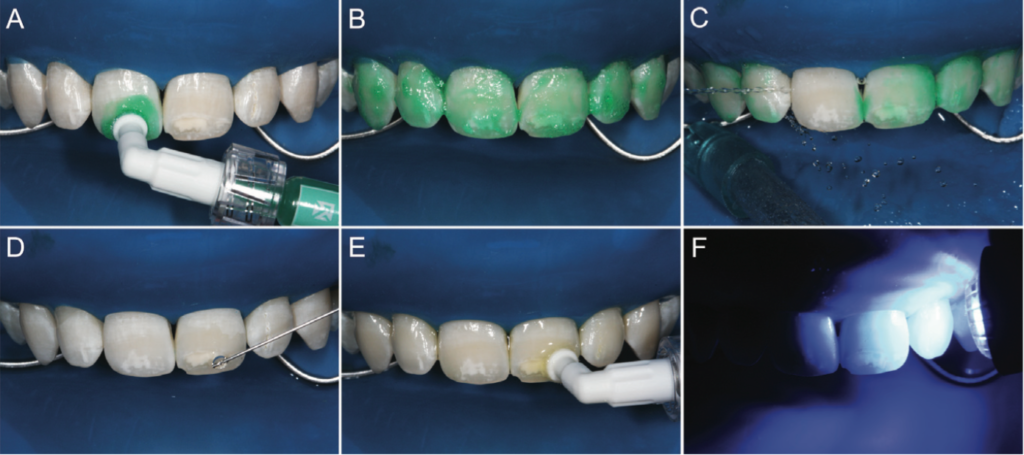
C, subsequently, the etching gel is thoroughly washed away (30 seconds) using water spray; D, lesions desiccated by application of ethanol (Icon-dry, DMG) for 30 seconds and subsequent air-drying; E, application of the resin infiltrant for 3 minutes (Icon-infiltrant, DMG); F, after removal of surplus material, the area is light-polymerized for 40 seconds. After this, a second coat of the resin infiltrant is applied, and it was polymerized (or light-curing) after a 1-minute delay.


Resin infiltration for arresting caries has been thoroughly studied, but now we are starting to understand its benefits for treating hypomineralization lesions. Due to the resin’s low viscosity, low contact angle on enamel, and high surface tensions, we can have high penetration into the capillary structures of the enamel body.
This provides a very conservative treatment option to solve an important problem for the patient.
The cases presented were completed and reported by MIGUEL ANGEL MUÑOZ, DDS, MS and LUIS ALFONSO ARANA-GORDILLO, DDS, MS.
The Morning Huddle has no affiliation with the the materials used in this article.