

Extraction is the only treatment option for a hopeless tooth caused by severe periodontitis. Once extracted, we are left with the options of implant restoration, fixed prosthesis, or removable prosthesis. All of these options involve considerable investment of time and money for the patient.
Intentional replantation of a tooth is a procedure most often done in endodontics. When a tooth with refractory periapical periodontitis cannot be treated with conventional root canal therapy (due to anatomical abnormalities, root fracture, or device separation), intentional replantation is an option, following in-vitro root canal therapy. In fact, severe periodontitis was considered a contraindication to intentional replantation.
However, if somehow intentional replantation could be a treatment option for periodontal hopeless teeth, it would be incredibly beneficial for the patient. With intentional replantation there are no immunological rejections due to foreign body presence. The treatment would be considerably shorter and lower cost. And the main complications would be tooth ankylosis or root resorption. In fact, ankylosis could improve the bone density of the area, which could be beneficial for implant placement, if the tooth needs to be extracted eventually.
How can we re-implant periodontal hopeless teeth to extend function?
Zhang et al. employed a procedural protocol to do exactly this, for 48 patients and 48 hopeless teeth.
- The patient had no systemic contraindications for periodontal surgery.
- The probing depth of the hopeless teeth reached the apex and the teeth had grade 3 mobility.
- The mobility of the adjacent teeth was less than grade 2.
Treatment
- First all patients had non-surgical periodontal treatment 2-4 weeks prior to intentional replantation.
- If the tooth had pulpal symptoms, root canal therapy was done before the extraction of the tooth (to relieve the patient of pain). If no pulpal symptoms were present, but endodontic infection was present, in-vitro root canal therapy was done following extraction.
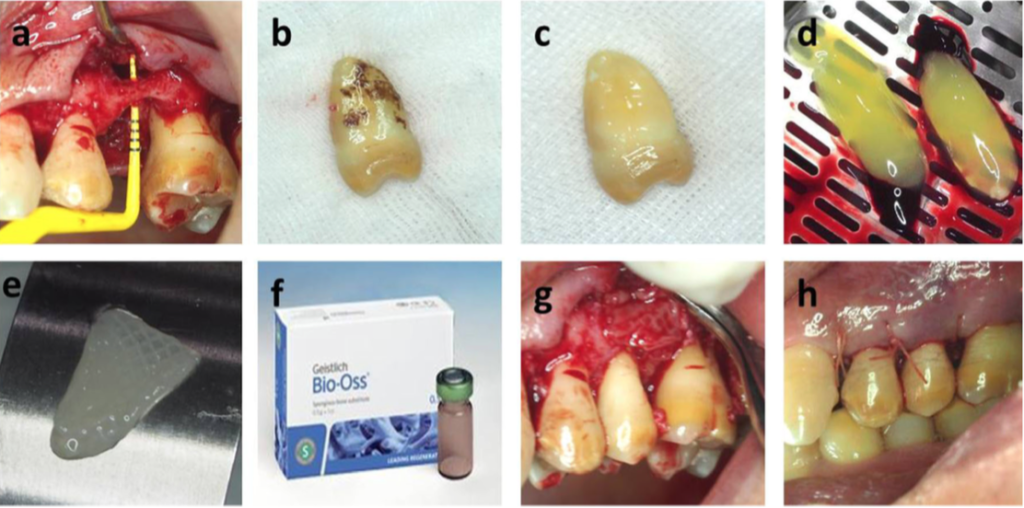
- Under local anesthesia, a mucoperiosteal flap was placed and the tooth was extracted (Figure A).
- All calculus, pathological periodontal ligaments, and cementum attached to the roots were removed with a Gracey curette (Hu Friedy, USA) (Figure b and C).
- The root surfaces were treated with 12% EDTA for 5 minutes and flushed with saline for 1 minute, the placed on a gauze soaked in saline.
- 9-10 ml of blood was drawn from the patient’s forearm and was centrifuged for 15 minutes. Following centrifugation, the upper layer of pale yellow liquid was discarded (lacking platelets). The middle layer containing Concentrated Growth Factors (CGF) and the lower layer containing red blood cell colloids were separated and kept (Figure d).
- Bio-Oss bone powder (Geiger, Switzerland) was mixed with the CGF and platelet colloid.
- The alveolar socket was filled with the fresh blood/ bone powder mixture; the tooth was replanted, and covered with a CGF membrane (Figure e, f and g).
- The socket was sutured (Figure h).
- The teeth were fixed with Superbond splint to create mobility grade 1.
- Occlusal adjustment was done.
- Antibiotic prescription of amoxicillin for 5 days was given and 0.12% chlorhexidine rinse for 10 days.
- The patients were instructed to not use the replanted teeth for 3 months.
Postoperative results
- For anterior teeth, the survival rate was 100% at 9 months and 96.3% at 18 months. For posterior teeth the survival rate was 90.5% at 9 months and 85.7% at 18 months. This difference in survival rate between anterior and posterior teeth is due to lower occlusal forcer on anterior teeth.
- At 18 months, the average mobility of the teeth was grade 1. 77.7% of the teeth showed evidence of ankylosis (accounting for the decrease in mobility).
- The periodontal pocket depth decreased significantly by 9 months and 18 months.
- Bone loss decreased at both 9 months and 18 months.
- There was an increase in gingival recession at 18 months.
- Smoking significantly decreased the survival rate of the replanted teeth, and mobility was higher for smokers.

Why the procedure worked
The bone powder used provides a porous scaffold for osteoblasts to migrate to the root surface, allowing the bone powder to be replaced by human bone. The CGF used is rich in many growth factors, and it promotes osteogenesis and wound healing following the replantation procedure.
Ankylosis was the main reason for the decrease in mobility of the replanted teeth. As the teeth were debrided before replantation, there was direct contact of the root surface with the alveolar socket. Because of this debridement, there was no periodontal ligament left, and therefore the teeth could not heal with periodontal attachment. Root resorption should be expected through this method.
With intentional replantation, we can extend the life of a periodontally hopeless tooth, reduce it periodontal pocket depth and its bone loss.