

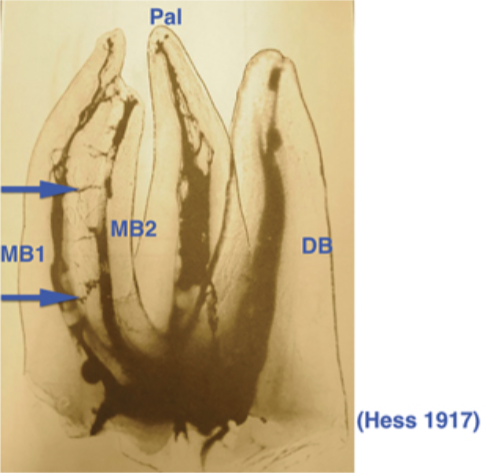
In 1917, Walter Hess first showed the presence of the MB2 canal. 90%-95% of first maxillary molars have been shown to have a MB2 canal. The identification and treatment of the MB2 canal is particularly challenging. However, leaving this canal untreated consists of an incomplete root canal treatment, which can propagate apical pathology, with the patient remaining in pain and the tooth in an infected state. As shown by Dr. Hess, the communication of MB1 and MB2 canals through isthmuses and anastomoses is evident. Therefore, if there are bacteria present in the MB1 canal, we can almost be sure that bacteria are also present in the MB2 canal.
Location of the MB2 canal
- Magnification and illumination during the procedure is critical, either with loupes or a dental microscope. Without these aids, MB2 canals are located 41% of the time, and with these aid – 94% of the time.
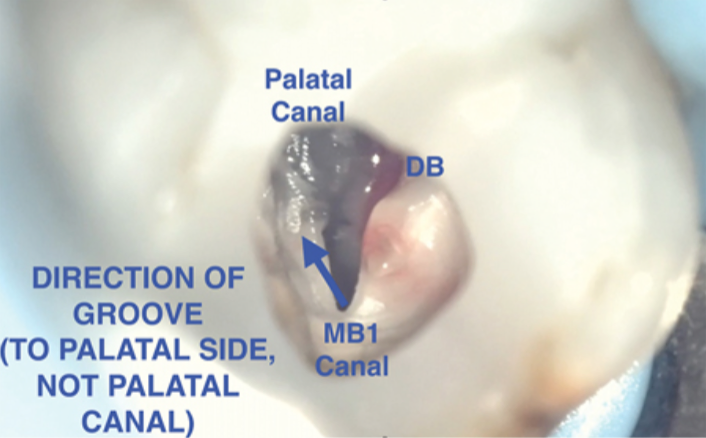
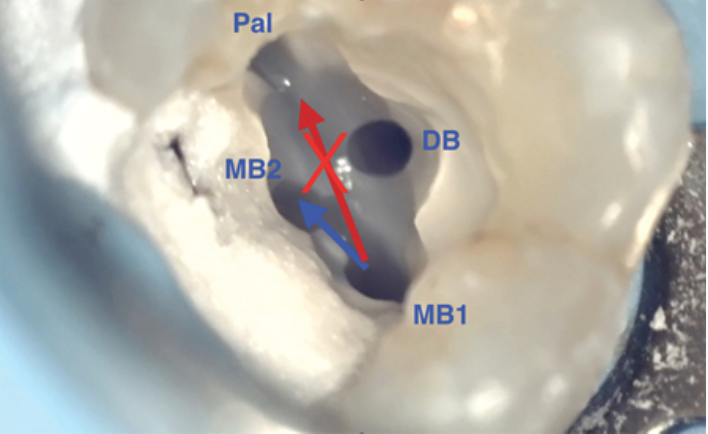
- The MB2 canal is most often located 1-3 mm from the MB1 canal, towards the palatal aspect of the tooth (not towards the palatal canal). In maxillary second molars, the MB2 canal is closer to the MB1 canal, when compared to first molars.
- Often, the MB2 can be hidden underneath a dentin shelf, especially in middle aged and older patients.
- The dentin shelf can be removed with the use of a slow-speed handpiece with surgical length round burs or a Mueller bur.
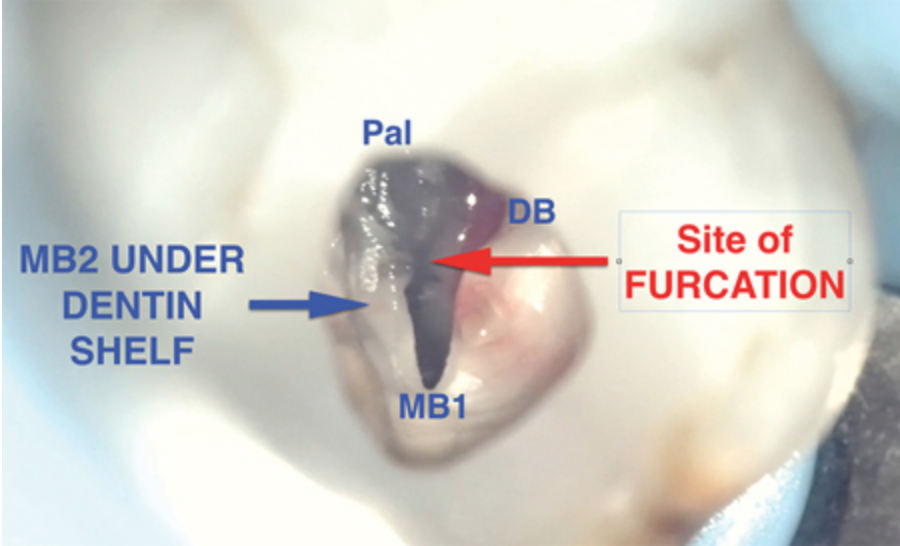
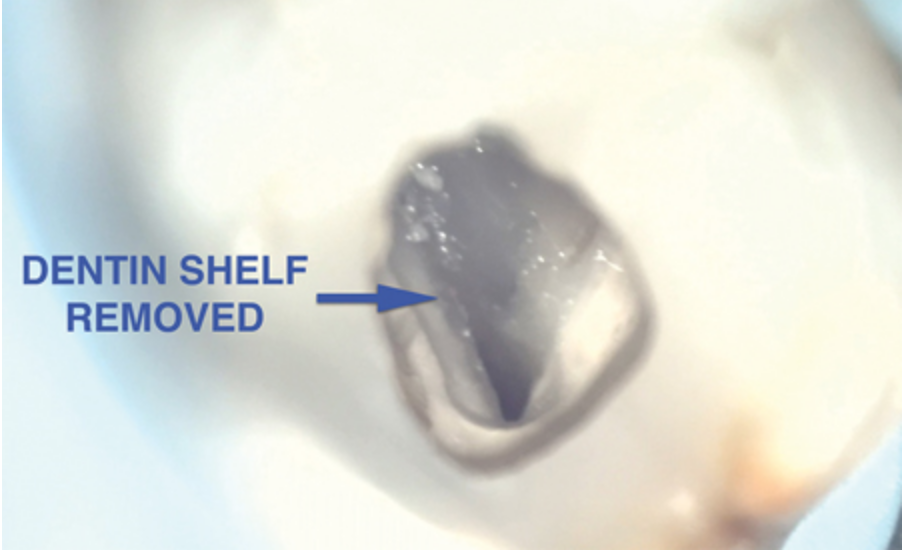

The direction of removal of the dentin shelf should be away from the MB1 canal, towards the palatal direction, but not towards the palatal canal. Drilling too far mesial, distal or towards the palatal canal can easily lead to perforations, especially in the furcation of the tooth. Since the MB2 canal is not located in the area of the furcation, that area should never be prepared in order to avoid perforations.
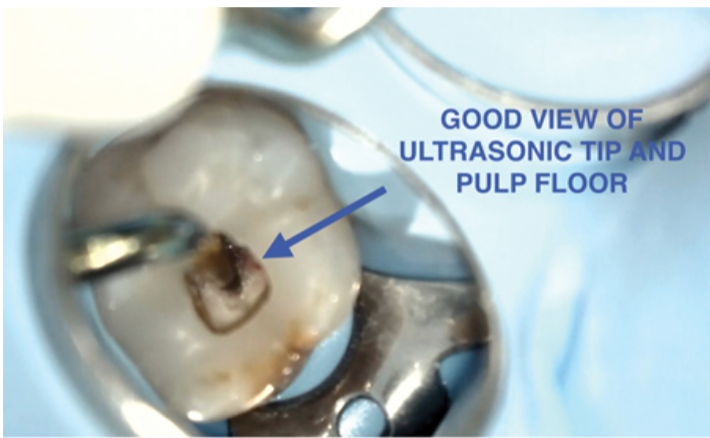
- The head of the slow-speed handpiece can block your view during the procedure. Ultrasonic tips make visualization much easier, and lower the risk of perforation.
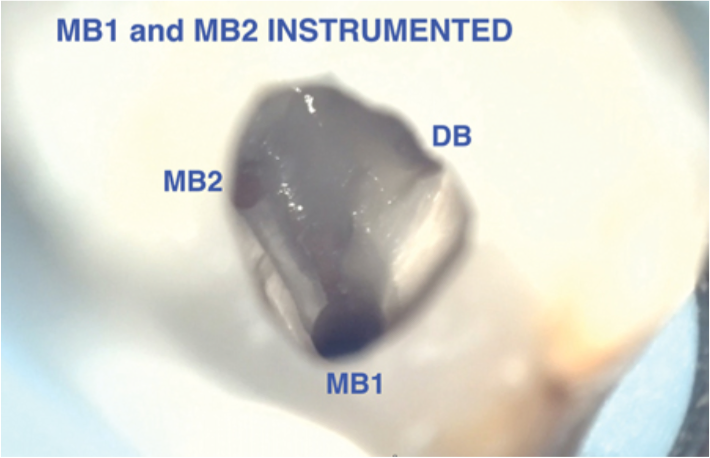
- As many MB2 canals can be small and calcified, they should be first instrumented with a small stainless-steel file and then NiTi mechanized files.
This demonstration was completed by Dr. Manor Haas, DDS, Cer. Endo, MSc(D), FRCD(C) and also published in Oral Health.