

Clinical Case Report
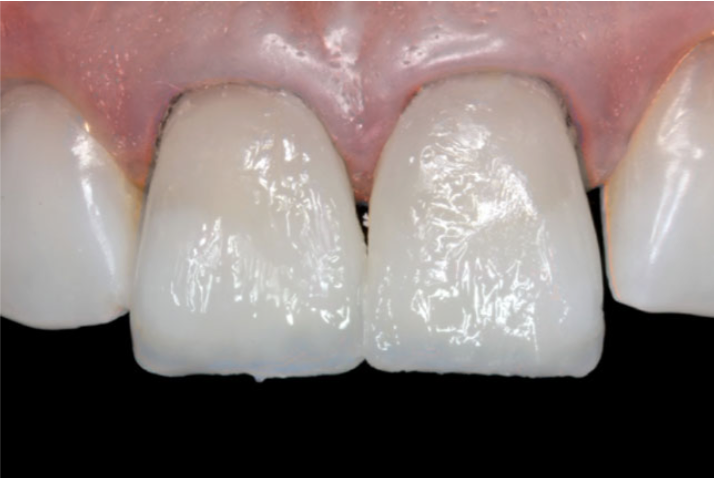
A 30-year-old woman presented to the dental clinic to improve her smile, because of multiple spaces between her anterior teeth.
- The patient is a heavy grinder, leading to generalized attrition and uneven anterior incisal edges.
- The patient had discolored cervical bonding on multiple anterior teeth.
- The patient did not report any medical history or medication usage.

Treatment
Before any “smile makeover” was started, a periodontal treatment was completed due to local gingivitis. This included education, oral hygiene instructions and ultrasonic plaque-calculus removal. This was done to achieve stable periodontal soft tissues.
Take home bleaching was done (4 hours/day for 15 days) to homogenize the color of the teeth – using Opalescence PF 10% Regular, Ultradent. The shade of the teeth transformed from A3 to A2.
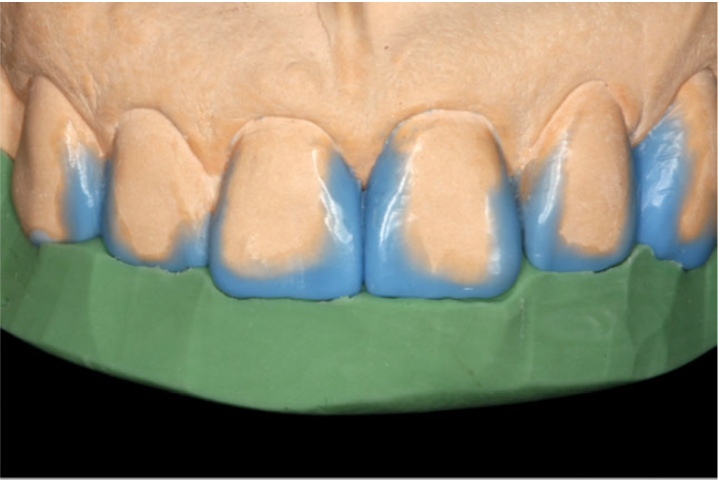
Following bleaching, upper and lower arch impressions were taken for analysis of the occlusal relationships, esthetic constraints and fabrication of wax-up of the final restorations. No contributory occlusal factors were shown and a silicone lingual index/matrix was made from the wax-up.

The shades of the final restorations were selected using the Vitapan Classic shade guide, while trying different composite shades intra-orally, when curing and wetting the various composite shades with saliva. A final 3D layout of the layering of the different shades of composite was made.

During the restoration procedure, all teeth were first roughened with a diamond bur, followed by applying 35% phosphoric acid for 30 seconds. The etch was rinsed with air-water and gently dried. Adapter single bond was applied to the teeth to the etched enamels for 15 seconds, air-thinned and light cured for 30 seconds. A second layer of adhesive was applied with the same protocol.
For restoring the anterior teeth, a “lingual-to-buccal layering technique” was performed. The first layer of enamel composite resin was applied to the palatal surface using the silicone index. Its important to note that the first layer of enamel composite should not be more than 0.5 mm in width, in order to avoid reduced space available for the subsequent composite layers. The first layer was cured for 5 seconds, followed by applying flowabale composite (with the same shade) at the tooth- composite interface to strengthen that portion. This was now cured for 40 seconds.
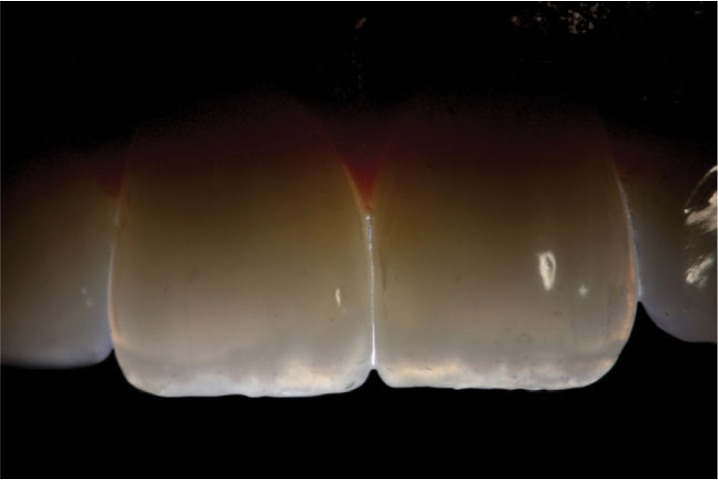
Now we get to the portion of the restoration that can take the final results from “good to great.” Following the enamel composite, several layers of dentin composite were placed and shaped to mimic dentinal mamelons. An incisal halo was created using a thin layer of composite of high value (Filtek Supreme XT, WE shade), and an oplascent effect was made using an effect composite (Filtek Supreme, Amber Translucent).



Finally, overlying these layers of composite, a final layer of enamel composite (same as the palatal) was spread over the buccal surface of the tooth. This composite was sculpted and blended with a sculpting brush to make an invisible margin between the restoration and the tooth. The tooth was finally cured for 60 seconds.
The same protocol was used for restoring all other anterior teeth. The teeth were shaped and polished with diamond burs, polishing discs and interproximal strips. The restorations were finished with foam cups (Enhance Polishing Cups, Dentsply) and polishing paste (Prisma Gloss, Dentsply) to obtain a natural gloss.

By using a direct restoration method with composite resin, we can achieve a predictable, minimally invasive and cost-effective treatment. Using a wax-up, silicone index and layer method, it is astonishing what we can produce with composite resin.
The durability of anterior composite resin build-ups is 85% in 5 years, indicating a stable and predictable result. Most of the incidences of failure are due to composite chipping or marginal staining. Composite chipping can be fixed with simple bonding and marginal staining can be avoided with blending during the initial restoration. By using this minimally invasive method, we still have the option to apply crowns and veneers in the future if need be. In the meantime, this patient has a completely new smile just with resin composite.

This clinical case was completed and reported by Abelardo Baez Rosales and Diego De Nordenflyncht Carvacho – Universidad Andres Bello, Vina del Mar, Chile.