

Following the extraction of a tooth, we can expect short-term and long-term resorption of the hard and soft tissues. Even with bone grafting of the extraction socket, there is still 1-2 mm loss of volume. This loss of volume is increased when we delay implant placement or socket preservation, leading to more invasive procedures being needed to reconstruct the lost tissues.
Recombinant technology has paved the way for synthetically engineered human growth factor. Recombinant human morphogenic protein-2 (rhBMP-2) has shown incredible results for socket preservation, sinus elevation and periodontal regeneration. Recombinant human platelet-derived growth factor – BB recruits osteoblasts to the wound, promoting increased and faster formation of extracellular matrix. It also increased the vascular endothelial cell growth factor, which increases the new vascularization of the extraction socket.
This is the next step in allowing ridge augmentation in the least invasive method possible. This is incredibly important and useful in the esthetic zone, where discrepancies of a few millimeters can disrupt the facial esthetics of a patient.
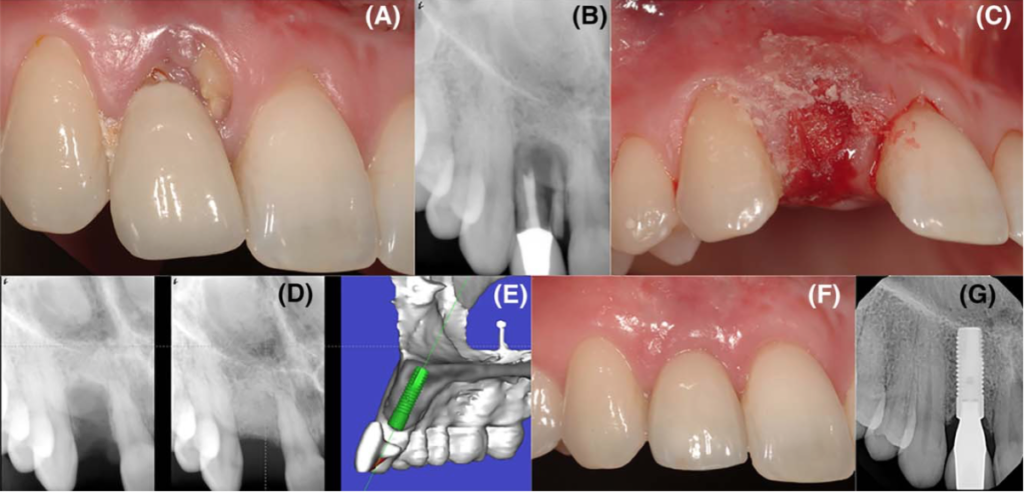
We can now highlight two cases with a single protocol that show how this technology can be used to preserve the alveolar ridge. This is done in a “flapless” technique (even when significant bone loss is present, even possibly compromising the buccal plate), critical for esthetic success in the anterior arch.
Procedural Protocol
- Pre-surgery patients were prescribed 1750 mg amoxicillin followed by 875 mg amoxicillin 2 x day for 5 days. If allergic, patients were prescribed azithromycin 500 mg 1 x day for 3 days.
- Following local anesthesia, the non-restorable tooth was extracted as atraumatically as possible using piezo-ultrasonic instrumentation (Piezosurgery Inc) and forceps.
- The extraction socket was debrided and granulation tissue removed with spoon curettes and more piezo-instrumentation. The socket was also irrigated with sterile water.
- 1g of freeze-dried bone allograft (Regeneross Particulate Allograft, Zimmer Biomet) was mixed with 0.5 mL of rhPDGF-BB (Gem21s, Osteohealth) and sterile water, and allowed to sit for 10 minutes.
- The bone matrix was now incrementally compacted into the extraction socket, overfilling the socket respective to the gingival margin.
- The socket was covered with a collagen membrane (Bio-Gide, Geistlich Pharma), which was trimmed to be fitted to the area and sutured.
- Patients were prescribed ibuprofen 600mg q6h, and follow up appointments were kept 1 week and 3 weeks following surgery.
- Following 5 months of healing with a provision prosthesis, implant surgery was started.

| The procedures and cases were completed and reported by Dr. Marc L. Nevins DMD, MMSC, and Dr. Sherif Said BDS, MSD, CAGS. |