
")
Conventional extraction techniques, using only elevators and forceps cause immediate and long-term changes to ridge integrity. Immediately following extraction, we see buccal plate fracture in 10% of cases, dehiscence in 28% of cases, and even buccal plate loss (4% of cases). In the long-term we can see ridge collapse 23% of the time. All these outcomes significantly alter any restorative treatment plans for that now-missing space. Clinical studies show that atraumatic extraction methods significantly reduce alveolar bone resorptions.
In fact, it was this very problem of resorption that lead Hürzeler et al. to introduce the socket shield technique for immediate implant placement. By sectioning and keeping a buccal fragment of a tooth, we can prevent buccal cortical bone resorption, and keep esthetic form.
From the patient’s standpoint, sectioning provides a more comfortable post-operative state – even in the most difficult extraction cases. For example, in a study of horizontally and buccally impacted mandibular third molar extractions, sectioning the teeth into three pieces prior to extraction significantly reduced post-op swelling, pain and trismus. Sectioning the tooth even reduced the treatment time. Happy patient, happy doc, happy practice.
Using atraumatic extraction techniques like tooth sectioning, can open up our options to predictably treat the most compromised patients. Dental extractions are a major risk factor for developing BRONJ, with its incidence increasing by 7X with conventional extractions. However, tooth sectioning prior to extraction has shown to significantly reduce the risk of BRONJ in patients getting bisphosphonate treatment.
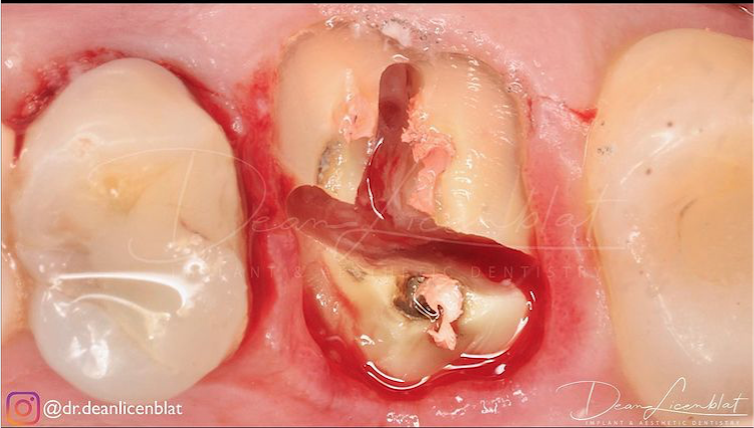
How To Section A Tooth
An extra step in the sectioning the tooth for removal is first amputating the crown of the tooth. This allows us to gain a direct view of the root anatomy of the tooth, therefore minimizing the amount of surrounding bone removed, and therefore reducing post op swelling and pain.




Tips From Dr. Licenblat
- “I use a 12 bladed tungsten carbide for sectioning teeth & course diamond to section crowns. Often I will decoronate with a diamond bur & section with TC. If I can see the dentine below the crown margin I will decoronate with TC under this and then section.”
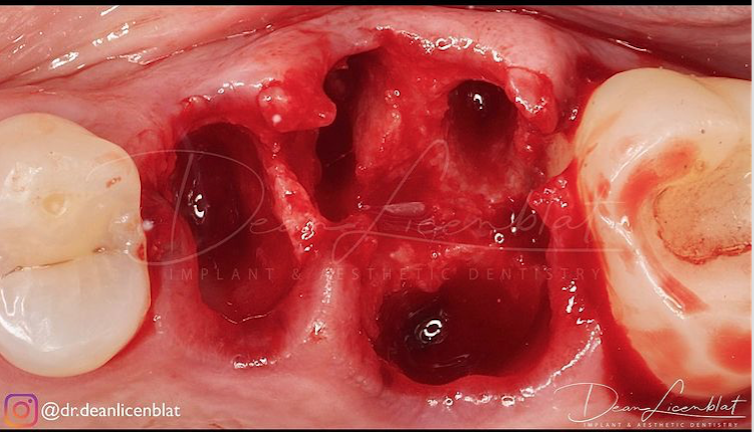
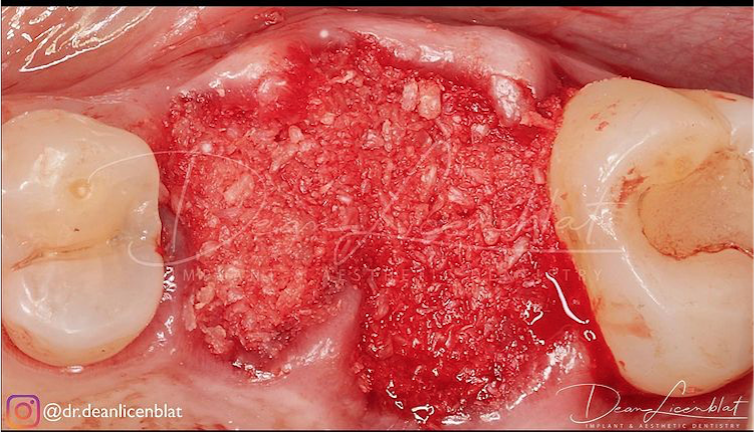
- “I am extremely conservative with the interradicular bone as this is a great source of blood and nutrients via angioneogenesis to your graft material. The more interradicular bone you have the greater your regenerative potential thus, you will have greater bone volume, greater bone height & better quality bone.”
- “By sectioning I see less debris around the site, less pain, post-op discomfort & contour loss as there is less alveolar fracture which results in bone loss. Furthermore, I feel the procedure is actually faster, better tolerated by the patient and I am significantly less likely to need to go fishing for broken root fragments.”
This Morning Huddle was brought to you by Dr. Dean Licenblat – Sydney, Australia.
Instagram – @Dr.deanlicenblat