

Patients being treated with anti-resorptive and anti-angiogenic medications have a risk of developing medication related osteonecrosis of the jaw (MRONJ). This condition can be more prevalent as a result of dental procedures which impact bone, such as simple extractions.
Patients at Risk
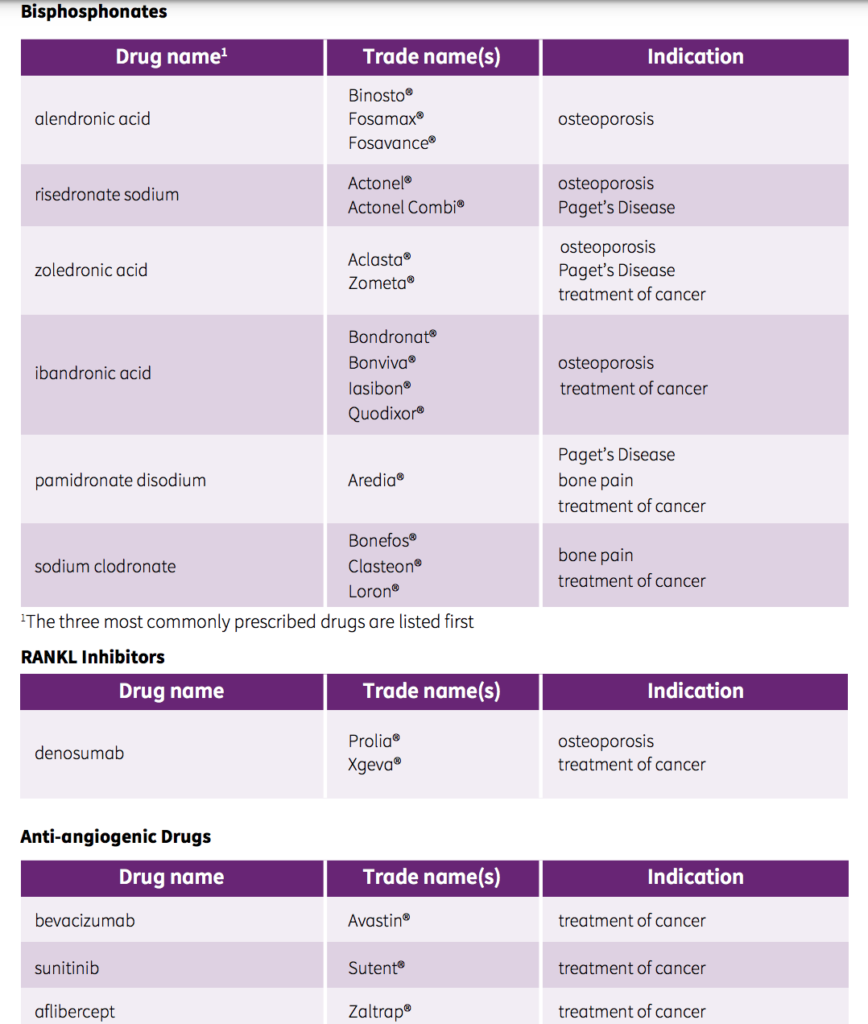
Anti-resorptive medication (such as IV bisphosphonates) are used to manage cancer related conditions associated with bone metastases in patients with solid tumors such as breast, prostate, and lung cancers and also lytic lesions resulting from multiple myeloma. Anti resorptive medications are also used for treatment of osteoporosis and osteopenia. These medications reduce bone resorption by way of osteoclasts and can have a positive effect on the quality of life of patients by reducing bone fractures and bone pain, however can increase the risk of MRONJ in patients.
Anti angiogenic drugs interfere with the formation of new blood vessel and are used in cancer treatment to restrict tumor vascularization. These medications also increase patient’s risk for MRONJ and are sometimes prescribed complementary to anti-resorptive medication.
Patients undergoing cancer treatment with anti-resorptive/anti-angiogenic medication are considered at significantly higher risk than those being treated for osteoporosis. However, treatment of osteoporosis with anti-resorptive medication for over 4 years and/or simultaneously taking glucocorticoids increases the risk of the patient to developing MRONJ.
MRONJ
Medication Related Osteonecrosis of the Jaw otherwise known as MRONJ can be described as exposed bone exposed through intraoral or extraoral fistula in the maxillofacial region persistent for more than 8 weeks. The patient medical history is significant for current or previous treatment with anti-resorptive or anti-angiogenic medication. No history of radiation or metastatic disease of the jaw is noted for the patient.
Pathophysiology is not fully understood but believed to stem from the suppression of bone turnover and inhibition of angiogenesis, as experiences by patients receiving therapy with anti-resorptive and anti-angiogenic medication.
Patients with MRONJ may experience symptoms of pain, delay in healing, exposure of bone, swelling and numbness. It’s important to note however that symptoms vary and findings of MRONJ may be incidental.
Dental Management
Any dental procedure impacting bone including trauma from ill fitting dentures, dental alveolar surgery including simple extractions can increase the risk of MRONJ in patients undergoing treatment with anti-resorptive and anti-angiogenic medication.
The aim should be to get the patient as dentally fit as possible prior to commencement of medication. Good oral hygiene and regular dental care is important to preventing dental disease. In high risk patients, non restorable teeth may be treated by removal of crown and endodontic treatment of the residual roots. Educate the patient and discuss the risk of procedures involved. Consider seeking advice of an oral surgeon or other specialists in clinical assessment, treatment planning and ongoing management.
Final Thoughts
Throughout our day to day we interact with many patients who sometimes have complex medical histories. It’s our duty to establish medical readiness prior to providing any treatment. We are very likely to come across patients undergoing cancer treatment. And with new advancements in treatment, new medications are readily introduced to the market, which we may not recognize. A simple medical consult with the physician or the oncologist in such a case is warranted in order be able to provide the best care for the patient.