

Case Presentation
An otherwise healthy 27-year-old woman presented to the Oral and Maxillofacial Surgery outpatient clinic at the Montreal General Hospital five hours after having had tooth 2.8 extracted by her general dentist. She complained of pain over her left eye, intermittent unilateral blurred vision, and double vision, following the extraction.
- Symptoms began soon after the extraction of tooth 2.8, and progressively worsened over the next hours.
- Extra- oral exam showed swelling of patient’s left face, left periorbital ecchymosis, left subconjunctival hemorrhage and proptosis of the left orbit.
- The patient’s pupils were equal and reactive to light and accommodation.


Opthalmology Consultation
An urgent ophthalmology consultation was summoned and the ophthalmology team performed a comprehensive orbital and eye exam. This confirmed an elevated intraocular pressure (23 mmHg) and exophthalmometry of 29 mm (9 mm proptosis) of the left orbit.
CT Scan
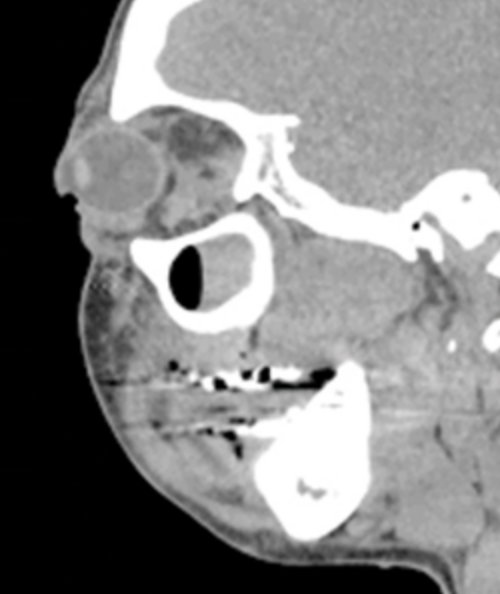
From this clinical presentation, an urgent computed tomography (CT) scan was obtained. The CT scan showed significant subcutaneous emphysema involving the left masticator space, which extended to the left eye through the inferior orbital fissure. The scan also revealed a 1.3 cm x 1.3 cm extraconal hematoma sitting above the superior orbital fissure causing minimal mass effect on the inferior and lateral rectus muscles.

Treatment
The diagnosis of a retrobulbar hematoma was made and the patient was then taken immediately to the operating room for lateral canthotomy, cantholysis and evacuation of the hematoma under general anesthetic.
- Hemostats are first used to devitalize the skin at the lateral canthus before the incision.
- Stephen’s scissors are used for the incision for the lateral Canthotomy. The incision begins at the internal aspect of the lateral canthus and extends approximately 1 cm to the lateral bony rim of the orbit.
- Retraction of the lower eyelid to expose the inferior aspect of the lateral canthal tendon. The anterior-inferior limb of the tendon is then cut with scissors.


Once awake in the recovery room, the patient reported an immediate relief of pressure and pain. The ophthalmology clinical examination performed the day after surgery revealed resolution of visual blurring and binocular diplopia. Over the course of the next two days, the ophthalmology findings returned to normal with complete resolution to normal vision.
Explanation
One possible mechanism would be that trauma from the dental extraction caused bleeding from the posterior superior alveolar artery, or from the pterygoid plexus of veins into the pterygomaxillary tissue and infratemporal space. From here, the bleeding could continue to tract into the pterygopalatine fossa and then toward orbit via the inferior orbital fissure.
The hematoma will cause a forward displacement of the globe (seen clinically as proptosis) and more significantly, will cause compression of the optic nerve and/or retinal artery that can lead to blindness.
It has been reported that blindness can actually occur within 90 to 120 minutes once compression and ischemia of the optic nerve has occurred.
A retrobulbar hematoma is a medical emergency that requires a prompt diagnosis and urgent care via either surgical decompression (lateral canthotomy and cantholysis) or medical management.
Today’s Morning Huddle was brought to you by Dr. Julia Pompura DDS, Dip OMFS, FRCD(C), Omar Bin Suhaym – R3 in the Oral and Maxillofacial Surgery Program, McGill University, Osama Alghamdi DDS, FRCD(C) – attending staff and Faculty at McGill University. This case was also initially reported in Oral Health.