

Amalgam tattoos in the esthetic zone is a tricky problem to solve.
Recent research shows that superficial pigmentations can be treated easily with lasers. However, deeper tattoos can involve soft-tissue, bones and periosteum – as can be seen in areas with endodontic amalgam retro- fills.
Case Report
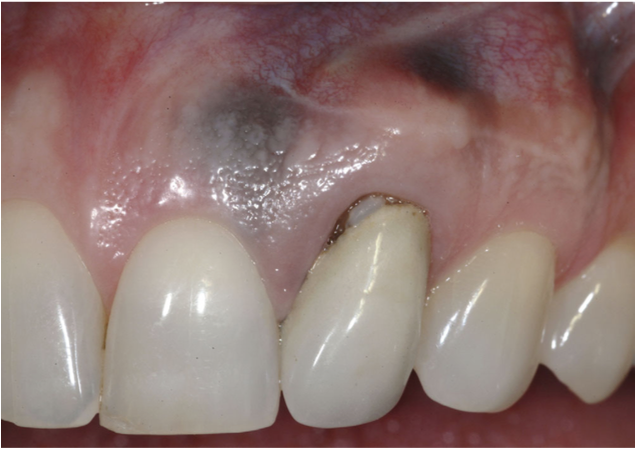
- A 45 years old female presented to the clinic with a chief concern of discoloration on her upper anterior gingiva.
- The patient presented with a high smile line, and discoloration only in the attached gingiva.
- There was history of amalgam retrofill on tooth #2.1.
- #2.1 also showed gingival recession causing it’s margin to be more apical compared to that of #1.1 and #2.2.
Treatment Summary:
The treatment plan was to eliminate the amalgam tattoo in the keratinized tis- sue, and move the gingival margin on #10 coronally for a more esthetic appearance.

Treatment Details:
The crown was first removed and a temporary restoration with placed leaving 2mm of root exposure, so that the gingival margin can be moved more coronally.

- Using the “tunneling technique,” a CTG was harvested and placed apical to the mucogingival junction of #1.1 and #2.2. A very wide graft was used in order to be able to cover the CEJ and the mucogingival junction at the same time.
- The donor site was covered with a plastic stent and the patient was given non-norcotic medication for postoperative pain.

Four months later, as the graft had matured, a coarse ball diamond bur was used to remove the stained portion of the keratinized tissue, and a surgical dressing was placed.


- 3 months later, the tissue appeared normal and the patient returned to have #2.1 permanently restored.
- A 14 year follow up showed that the amalgam tattoo has not recurred, the gingival and final restoration margins showed to be stable.


This case was completed and reported by Dr. David Mathews, specialist in periodontics – Washington, USA.