

It’s Friday afternoon. You’re ready to go home. You’ve extracted a tooth on the maxilla, and now you see an itty-bitty hole in bottom of the tooth socket. Could it be…a sinus perforation?
This can lead to a lot of problems down the road for the patient. In fact, tooth extractions are not the only way oroantral communications (OAC) can happen. Dental infections, trauma, radiation therapy or osteomyeltitis can cause this communication as well.
This communication can obstruct the healing process of the tooth socket, and if the OAC remains open and becomes epithelialized, it turns into an oroantral fistula (OAF).
You should know that the extraction of maxillary 2nd molars cause the most OACs (45%), followed by 3rd molars (30%), 1st molars (27.2%), and finally 2nd premolars (5.3%).
Signs and Symptoms
These can vary form purulent discharge from the fistula to the patient’s own experiences of having oral liquids into the nostrils on the same side of the potential communication. However, some patients may not present with any of these findings. Yet, if left untreated, sinus communications can lead to infections, chronic sinusitis and impeded healing.
Diagnosis
If you ever suspect an OAC, don’t panic. Here is a quick reference decision tree to help you in your diagnosis.
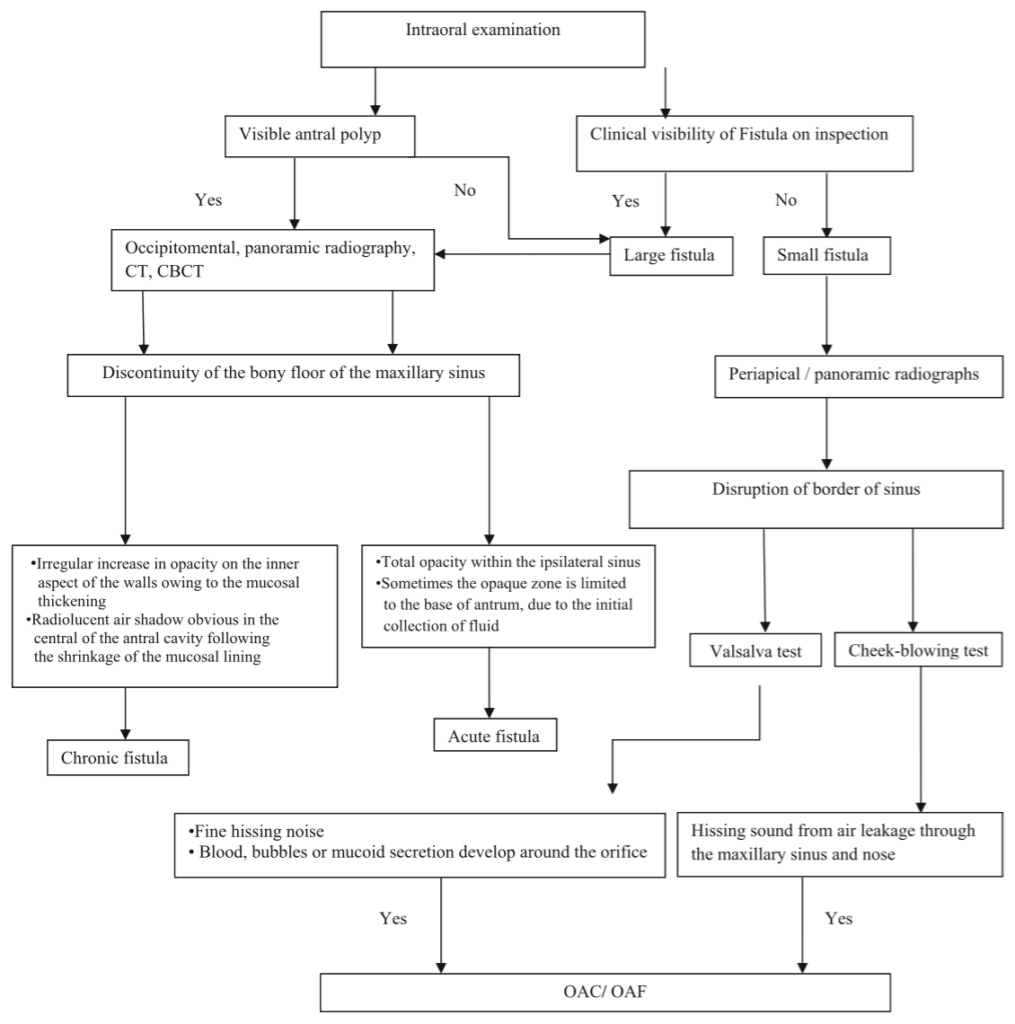
*Notes:
Valsalva Test – Named after Antonio Maria Valsalva, the 17th century physician. The patient is instructed to exhale through a blocked nasal airway. If an OAC is present, hissing or bubbling sound will present in the site of the communication.
Cheek-Blowing Test – The patient is instructed to blow air into the cheeks against a closed mouth. Caution: this test is considered a risk for antral complications due to the spread of microorganisms from the mouth to the maxillary sinus.
Today’s Morning Huddle is brought to you by Dr. Puria Parvini et al. – Frankfurt, Germany.