")
Immediate implant placement following tooth extraction is a predictable treatment with a high success rate. However, when it is done in the anterior esthetic zone, bone and gingival recession can be expected following extraction of the natural tooth. It has even been shown that this soft and hard tissue remodeling takes place, irrespective of if an implant is immediately placed or not. Unfortunately, many cases of immediate implant placement in the esthetic zone resolve with mid-facial gingival recession and an incomplete buccal bone wall. Dr. Juan Zufia and colleagues present a case where a single appointment soft and hard tissue augmentation is done, alongside immediate implant placement. This case shows predictable outcomes to counter the expected gingival and bone resorption.
Case Presentation
A 53-year-old patient presents with severe generalized periodontitis, with a chief complaint of a loose upper left central incisor. Clinical exam shows severe periodontal attachment loss around the central incisor, alongside bone resorption. The periodontal condition of the surrounding teeth is also dire and any fixed prosthesis is contraindicated.

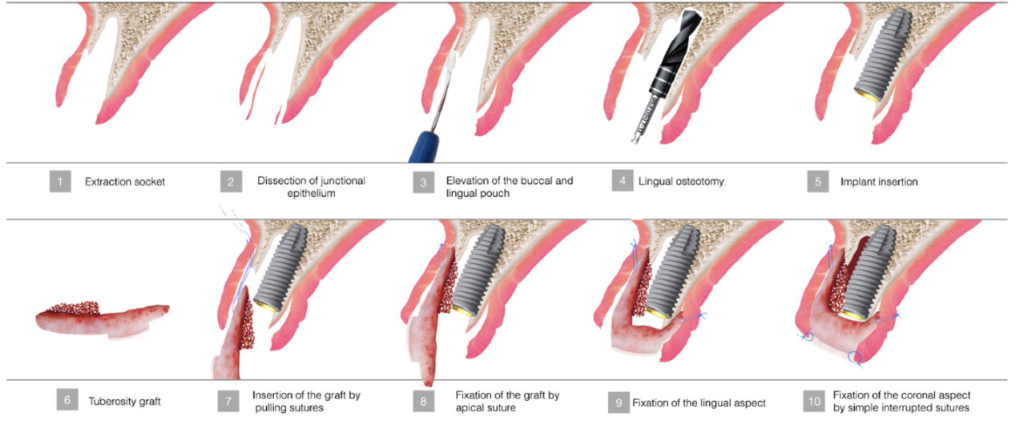
- The upper left central incisor was extracted, preserving the interdental papillae.
- The socket was debrided, eliminating all granulation tissue.
- Using a high-speed diamond bur and microsurgical blade, a supraperiosteal tunnel is made on the buccal and palatal aspects of the socket.
- The gingival and bone defects are measured with periodontal probe in order to determine the size and shape of the donor tissues needed.
- Considering the space needed to restore, an implant 4.3 mm in diameter and 13 mm in length (Camlog Screw Line) was used.


Four Layer Soft and Hard Tissue Graft – Following Implant Placement
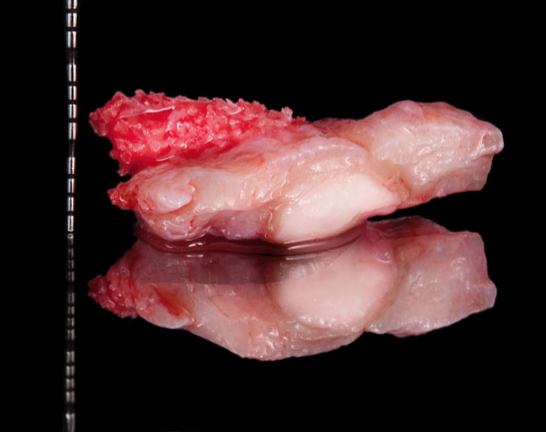
- A four-layer graft was harvested – a combined epithelialized-subepithelialized connective tissue graft and cortical-cancellous autogenous bone graft – from the patient’s maxillary tuberosity. A CBCT was taken prior to the procedure in order to determine the thickness of the receptor and the donor site, and to prevent perforation of the maxillary sinus.
- The four-layer tissue graft was harvested from the hard palate and the maxillary tuberosity and trimmed to match the size and shape of the receptor socket.
- The graft is introduced into the receptor socket by having the bone graft in the inner buccal aspect of the socket and the subepithelial connective tissue at the outer aspect. The graft is stabilized by apically placed buccal and palatal sutures.
- The site was temporized with a resin crown that was splinted to the teeth on either site of the surgical site.


Post-Op
- Chlorhexidine gluconate 0.12% 2x per day was prescribed, along side Ibuprofen 600mg 3x day and amoxicillin 500mg 3x day, for seven days.
- The patient was clinically monitored every 2 days for 2 weeks, and every 15 days for the next 4 months.
- Following 4 months, as no infection was seen, the implant was exposed and restored with a provisional implant supported prosthesis- in order to contour the soft tissues.
- At 6 months the implant was permanently restored with a zirconia abutment and an all-ceramic crown.
- The patient also underwent periodontal maintenance therapy every four months for 3 years.
This case shows how we can restore incomplete buccal bone and soft tissue height, without the use of any biomaterials, in a single procedure. Following 3 years of follow up, a great esthetic result was achieved, with no gingival or bone resorption.

This case was completed and presented by Dr. Juan Zufia DDS, Gonzalo Blasi DDS, MS, Ramon Gomez-Meda DDS, and Alvaro Blasi DDS, CDT. This case was also published in the journal of esthetic and restorative dentistry.