

Dental wear is the loss of hard tooth structure, from any etiology, other than caries or trauma. Usually it arises from erosion, abrasion, abfraction, or attrition. Although tooth wear is a normal physiological process, its aggressive progression can have a lot of consequences:
- Loss of vertical dimension, resulting in dento-alveolar compensation
- Tooth sensitivity
- Decreased quality of life
- Esthetic disturbances when altering the smile line or incisal edge position
- Loss of anterior guidance and canine protection, increasing the horizontal stresses on posterior teeth
Maxillary anterior teeth are the most commonly involved teeth when dealing with wear. This is accompanied by posterior dento-alveolar compensation, in order to attempt to preserve posterior inter-occlusal contacts and mastication systems. Carrying these processes years into the future, the patient ultimately ends up with an inadequate inter-occlusal space.
Restoring worn teeth should involve considering several factors:
- The pattern of maxillary anterior teeth wear
- Inter-occlusal space availability
- The space needed for the proposed restorative treatment
- The quantity and quantity of available dental hard tissues
- The esthetic goals of the patient
When treating wear or a collapsed bite, we are generally aiming to provide more overjet and/or less overbite. We generally have three restorative options:
- Increasing vertical dimension of occlusion (VDO), by restoring the occlusion of posterior teeth (either one arch or both). This restoration should be as minimal as possible
- Intrusion of maxillary and mandibular teeth with orthodontics, followed by restoration of those same teeth
- Restoration of posterior teeth in centric relation, in order to achieve restorative space for anterior teeth. This is to be done through articular analysis, and determining stability and patient comfort, when comparing the patient in CR or maximum intercuspation position (MIP)
Case Report
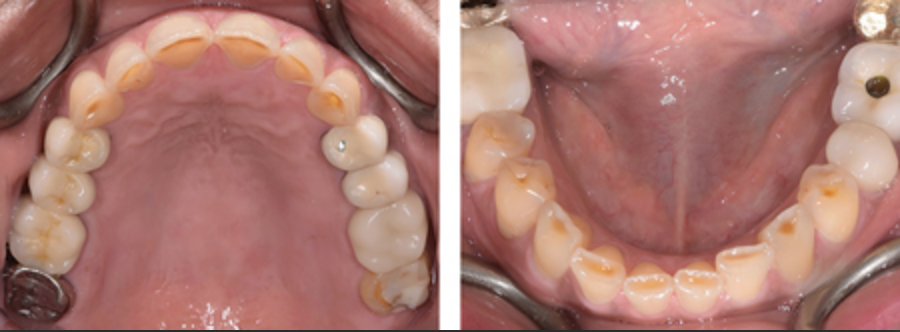
A patient presented due to wear of her anterior maxillary and mandibular teeth. The maxillary posterior teeth were already restored with metal-ceramic crowns, some of which had porcelain chipping and leaking margins.


Treatment Plan
- Replacing maxillary posterior crowns
- Placing new crowns on maxillary anterior teeth
- Direct resin composite restoration of mandibular anterior teeth
Initially an articulated diagnostic wax-up was completed to increase the VDO, therefore increasing the overjet and reducing the overbite. This was done to increase the occlusal space between the posterior teeth. This also allowed for enough space on the lingual of anterior teeth, not having to reduce excessive tooth structure during the crown preps.



| The final restorations were:Posterior zirconia-layered crownsAnterior E-Max crowns from canine to canineLower anterior incisal edges were directly restored with compositeA maxillary occlusal guard was fitted after final cementation Whenever increasing the VDO, it is critical to place the patient in temporary restoration for a “trial period.” This allows you and the patient to evaluate the shape/position of the new restorations, esthetics and phonetics. More importantly, if there are any fractures or signs of wear on the temporary restorations, we know that adjustment need to be made to the final restorations, to accommodate the patient’s functional patterns. |
| Today’s Morning Huddle was brought to you by Dr. Mario Rotella |