

Clinical Presentation
- 44-year-old woman presents to the clinic due to a lesion on the left lateral border of her tongue (17x10mm). The lesion shows a soft nodular swelling, circumscribed, with white irregular papillary projections. The lesion is non-indurated.
- The lesion has been present for 4 years and is asymptomatic.
- No significant findings in the patient’s medical history.

Differential Diagnosis
Since the patient was a healthy woman and the lesion was a long-standing asymptomatic lesion, a malignancy was highly unlikely. The differential diagnoses were limited to benign conditions.
- Granular cell tumor: a benign neoplasm with possible neural origin. Usually presents as single yellowish, non-painful, nodular swelling. This neoplasm is most often covered by normal mucosa. Most common sights are the buccal mucosa and the dorsum of the tongue. This lesion is predominantly found in women ages 40-60 years.
- Verruciform xanthoma: A superficial lesion caused by accumulation of foamy macrophages in the papillary connective tissue, giving it a sessile papillary appearance. These lesions most often are seen on the alveolar ridge, gingiva, and palate. Depending on the severity, the mucosa color can range from normal to white or yellow.
- Condylomata: caused by a viral infection, affects the skin and mucosa of the anogenital region and oral cavity. In the oral cavity, these lesions are most often seen on the lips, tongue and floor of the mouth.
- Verrucous hyperplasia: A precancerous lesion, which can present as a white or pink mass with a papillary surface. These lesions are usually seen on the buccal mucosa, tongue and palate.
With local anesthesia, excisional biopsy was done.
Histopathology
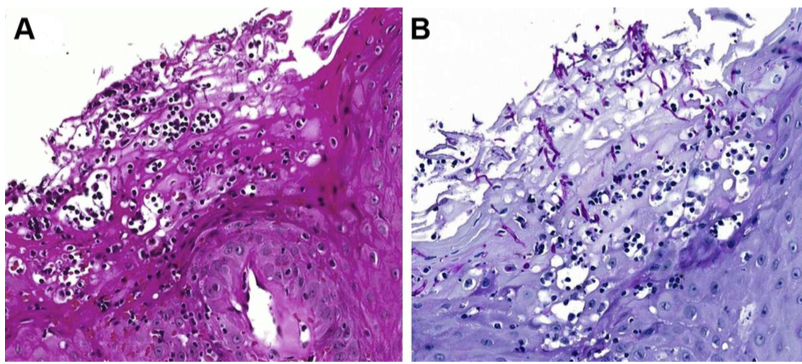
- Hyperplastic, hyper-parakeratinized stratified squamous epithelium with surface papillary projections.
- Lymphocytes and plasma cells were concentrated in the subepithelial layer.
- Intraepithelial collections of lymphocytes, polymorphonuclear leucocytes and cell debris.
- Periodic acid-Schiff (PAS) staining showed fungal hyphae in the epithelium.
Diagnosis
- Chronic hyperplastic candidiasis – nodular type.
Chronic hyperplastic candidiasis is an extremely rare oral lesion – a variant of oral candidiasis. It presents as a white plaque that can’t be rubber off. It usually appears in the buccal mucosa or posterior commissural region.
A candida infection can provoke a hyperplastic response forming a raised mass, as seen in this case. Because of this presentation, it can mimic a malignant lesion. The prognosis is good in the majority of cases. It has been studied that poor diet, emotional stress or high estrogen levels can promote fungal infections leading to such a presentation. Presence of candida hyphae in the histopathology is the critical diagnosing factor
Treatment
Complete excision of the lesion is indicated with this diagnosis. In this case, the patient underwent excision biopsy and no other treatment was needed. Following 6 months, no residual lesion was detected. Tongue mobility was within normal limits. Good oral hygiene was critical, to prevent recurrence of the infection. Antifungal therapy was not necessary as the entire lesion was removed during excisional biopsy.
This case was completed and presented by Dr. Alicia Rumayor Piña, DDS, MSc