
")
| The primary goal of any dental treatment is to preserve the pulp or reverse any damage to it. In mature teeth, when there is a carious pulp exposure, the usual treatment is pulpectomy or root canal therapy. The consensus is that pulp capping (most often performed using calcium hydroxide), whether direct or indirect, doesn’t lead to predictable and stable results. However, new research has shown that the pulps in mature teeth have a greater regenerative potential than what was previously thought. Tricalcium silicate-based materials (mineral trioxide aggregate, MTA) have proven to induce growth factors to induce repair in an inflamed pulp, through Vital Pulp Therapy (VPT). Given the superior marginal sealing ability of MTA, VPT has the potential to transform the management of carious exposures in mature teeth, compared to the poor marginal seal of Calcium Hydroxide. Furthermore, studies have shown that the technical quality of root canal treatments range between 30% to 60%, depending on the practitioner. The technically less challenging procedures of VPT provide a more predictable alternative. |
| Considerations for VPT in mature teeth Age: VPT has for the most part been restricted to younger age groups, however age does not appear to be a factor in the outcomes of VPT. Pulpal status: The use of MTA in cases of irreversible pulpitis have even resulted in predictable healing, showing that painful pulpitis is not a contraindication of VPT. |

To pulpotomy or not to pulpotomy:
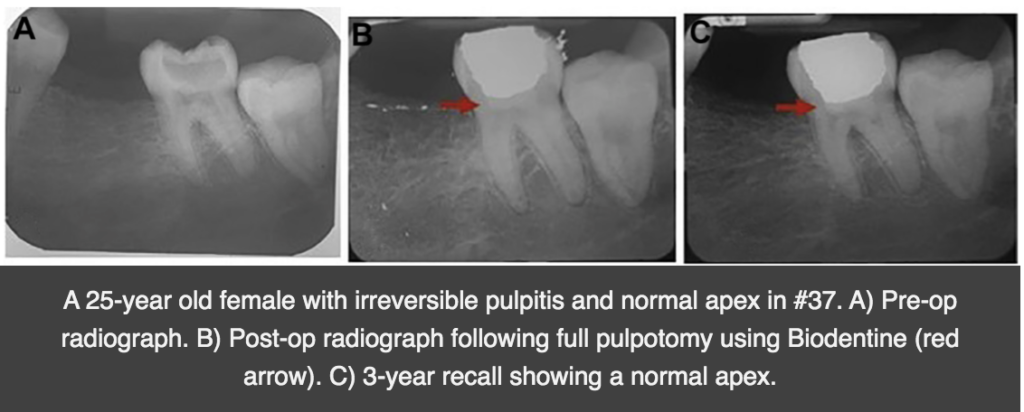
Presence of a periapical lesion in an inflamed vital pulp is not a contraindication of VPT either. Several studies have reported successful outcomes of pulpotomy in teeth with periapical lesions. However, when using VPT, any and all necrotic tissues, dental debris, or yellow areas within the pulp should be removed, in a partial or full pulpotomy. Pulps underlying a carious exposure will have a definite zone of inflammation beneath the exposure. Therefore, removal of the affected pulp is needed, rather than covering the inflamed portion of the pulp with material. Direct pulp capping with a partial pulpotomy in adult teeth has shown a success rate of 85% during 2-3 years of follow up, in teeth with reversible or irreversible pulptitis. If a full pulpotomy is done, the success rate has been shown to be 90%-98%. Moreover, the outcomes in systematic reviews have shown similar results between irreversible and reversible pulpitis, with the use of VPT.
Disinfection:
When the pulp is exposed, the cavity should be disinfected with 1% NaOCl to reduce the bacterial load, which can interfere with healing. Hemostasis can be achieved with 1%-3% NaOCl on a cotton pellet as well. After VPT, the restoration provides a good seal against micro-leakage.
Materials to use:
Hydraullic calcium silicate-based materials have shown much better outcomes than Calcium hydroxide. Calcium hydroxide has shown a low success rate of 35% when used in direct pulp capping. MTA can provide a non-staining fast set (12 minutes) option for VPT. They induce mineralization, cellular differentiation, and the release of dentin matrix components to promote angiogenesis and dentinogenesis. On the other hand, resin based materials or calcium silicate-based materials have shown negative outcomes on the pulp, and therefore should not be used.
| When it comes to the patient, with the use of pulpotomy and VPT, we can reach reduction of pain level close to 95%! VPT in mature teeth is a minimally invasive and cost-effective treatment of the inflamed tooth. A cost-effective analysis can show that vital pulp therapy can be more cost effective than root canal treatments. All the while, we are leaving the tooth functioning, hydrated and proprioceptive. The high success rate of this procedure of mature teeth makes this an attractive treatment option. |
| Today’s Morning Huddle is brought to you by Dr. Nessrin A. Taha, Jordan University of Science and Technology. |