
")
After practicing dentistry for a few years we are bound to come across different populations of patients, some of whom present with rare genetic disorders that requires unique management and careful planning in order to achieve a treatment outcome tailored to their needs. Ectodermal Dysplasia (ED) is a rare hereditary condition affecting structures of ectodermal origin including skin, hair, nails, teeth and sweat glands.
Common clinical findings including:
- Absence or reduction in number of sweat glands (hypohidrosis)
- Sparse light colored scalp and body hair (hypotrichosis)
- Hypodontia, flat bridge of the nose and prominent forehead, periorbital hyperpigmentation
Oral manifestations include:
- Partial or complete adontia
- Abnormal shape of teeth
- Enamel hypoplasia
- Atrophic and asymmetric alveolar ridge
- Maxillary retrusion and high palatal arch
Absence of teeth from an early age affects patients masticatory functions which can lead to avoiding certain foods and cause nutritional deficiencies. Speech will also be affected due to absence of teeth, and development of facial features will also be impacted. Proper prosthetic management in these patients is of utmost importance in order to support growth and achieve desired functional, aesthetic, and psychological outcomes.
Case Report
Patient: 5 year old Middle Eastern boy
CC: Multiple missing teeth
RMH: Patient diagnosed with Ectodermal Dysplasia
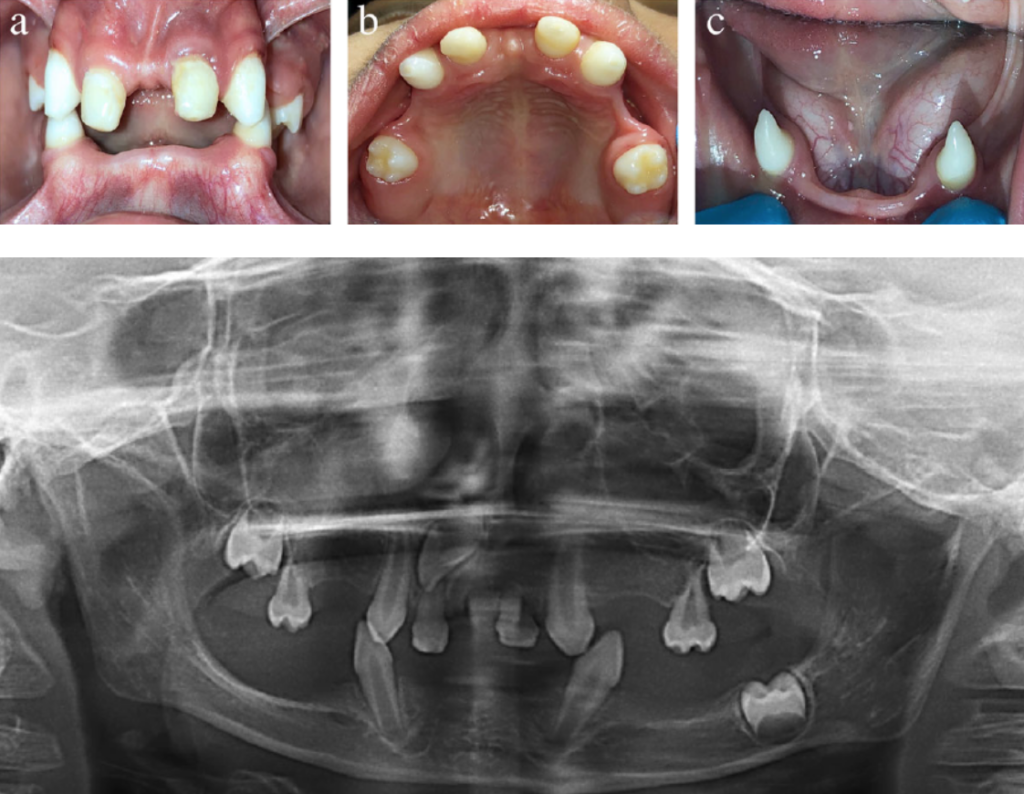
Intraoral Findings
- 8 teeth present including upper primary second molars, upper permanent canines, upper primary canines (shaped to look like incisors), lower permanent canines
- Deep overbite, Class 2 occlusion, contact only noted between upper and lower anterior canines
- Thin atrophic knife edge alveolar ridge with loss of vestibular height of mandibular arch
- Hyposalivation, viscous saliva contributing to plaque retention
Radiographic Findings
- Panoramic radiograph revealed four unerupted teeth: upper right first molar, upper right lateral incisor, upper left first molar, lower left first molar
- Reduced height of the mandible
Treatment Planning
- Removable partial dentures
- Overdentures
- Fixed partial dentures (FPDs)
Removable partial dentures are the most common treatment for children with oligadontia, however, these prosthetics often require much adjustments and are not well accommodated by young children, in addition to ridge deficiencies of the patient this option was excluded. Fixed partial dentures can provide a more patient friendly treatment option in improving mastication and speech function and may be more ideal in treating young patients with multiple missing teeth. The parents preferred a fixed prosthesis.

The final restorations were:
- Nance space maintainer -used as a provisional until eruption of the upper right permanent lateral incisors -designed with a saddle to replace upper primary first molars, single incisor added
- 8 unit metal ceramic bridge using the lower permanent canines as abutment, replacing incisors and primary first molars.
Upper arch was restored with nance appliance two weeks prior to delivery of the lower appliance in order to gradually open the bite and train patient in the new occlusion. Reestablishment of occlusion lead to increase in vertical dimension especially in the lower third of the face and increased lip support.
The future options for replacing the missing anterior teeth in the maxilla can include a conventional bridge extending from canine to canine, a maryland composite resin bridge, or modification of the design of the existing Nance appliance.
Instructions were given to patient’s parents for speech training. 6 months follow up revealed appliances were well tolerated by the five year old patient and improvements in speech, masticatory function were noted.
Today’s Morning Huddle was brought to you by Reema AlNuaimi and Mohammad Mansoor