

Case Presentation – Full report can be accessed here.
76-year-old male. Presents to the hospital due to headache and drainage of purulent discharge on right side of his face. Patient’s medical history indicated hypertension, alcoholism, and previous history of smoking. The patient was in a car accident three months ago, for which he was treated at a hospital with a pectoral muscle graft to reconstruct his facial defects.
Physical examination
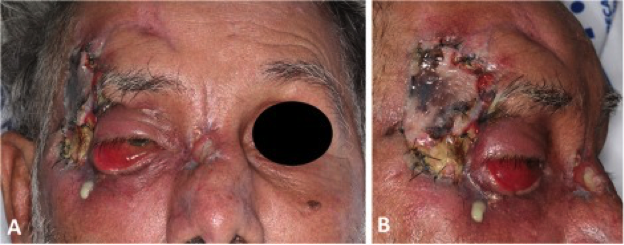
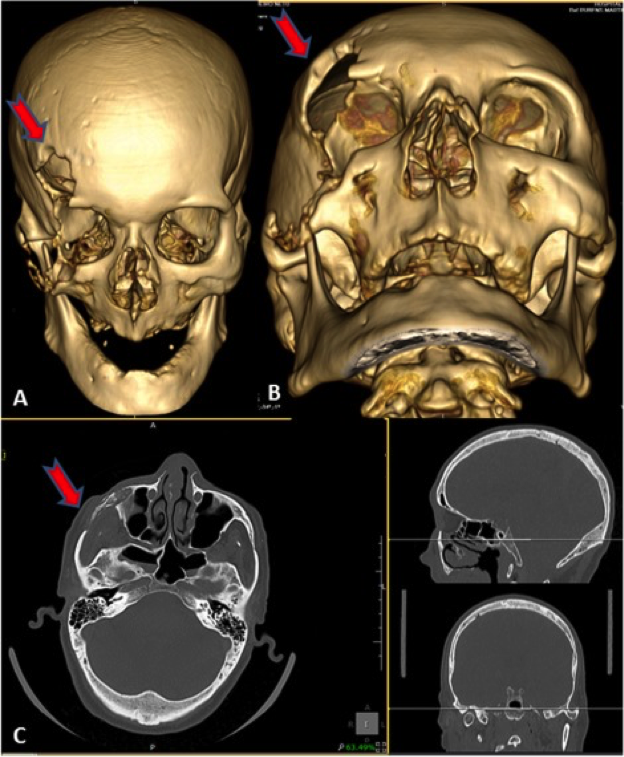
Lower right eyelid ptosis. Right frontotemporal graft showing hyperemic margins, necrotic coloration, with purulent secretions along with pain during palpation. Laboratory results showed no significant findings. Cranial tomography shows discontinuation of structures within the internal bone table, as the case with the dura-mater in the area. In addition, there was the presence of bone sequestrum.
Diagnosis
Craniofacial osteomyelitis – due to the presence of bone sequestrum and the results of the craniofacial tomography.
Multidisciplinary Treatment
The infectious disease team indicated an antimicrobial regiment of 6 weeks comprising of Vancomycin, Cefepime, and Clindamycin.
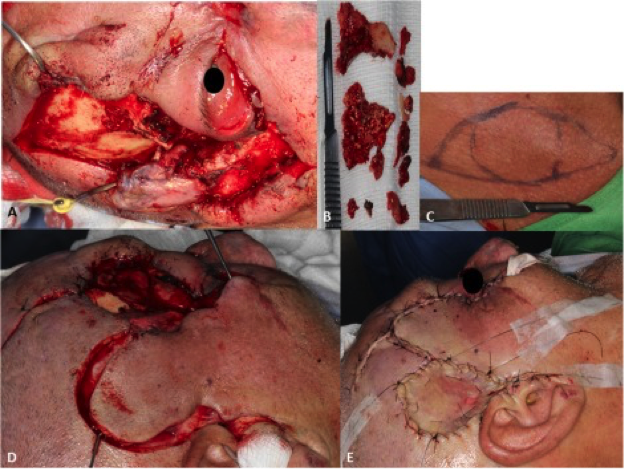
A multidisciplinary team consisting of OMFS, neurosurgery and plastic surgery, using general anesthesia – performed debridement of the osteomyelitis, alongside craniofacial osteotomy in the frontotemporal region and right zygomatic bone. A supraclavicular free graft was also performed to correct the defect present along the region. Necrotic bone was sent for antibiogram testing and culturing.
Post op
The patient was kept in the hospital for 39 days, to promote healing, provide dressing and drainage of the region. Following no pain symptoms, no signs of new infection, and good blood perfusion to the graft, the patient was discharged. Outpatient follow up was done 15,30, 60 and 360 days – with the only complaint being the right eye ptosis of the patient. Annual postoperative control appointments were indicated for the patient.

Discussion
The inflammation of bone is known as osteomyelitis. This inflammation is usually due to bacterial infection of cortical bone, trabecular bone, periosteum or the bone marrow. This can happen after trauma or radiation to the area. Due to not having any hallmark symptoms, diagnosis of osteomyelitis is particularly difficult, and multidisciplinary in nature. Laboratory and histopathological testing is necessary, alongside with imagining. It can present with fever, pain and/or drainage. Thorough debridement of the infected bone and tissues is essential along side antibiotic therapy. Following stabilization of the infectious state, restoring bone and soft tissues can be done, with the challenge being maintaining vascular perfusion to the area. This is particularly important, as antibiotic supply to the bone is essential.