
")
When placing implants in the esthetic zone, the response of the peri-implant soft tissue is just as important as the final restoration. What creates a pleasing smile is not only the size and shape of the teeth, but also the frame that they’re held in – the gingiva. The margin, color, texture, and height of the interdental papillae should match that of the existing dentition.
To create the ideal gingival structures around an esthetic-zoned implant, we can control the timing of the implant placement and the timing of the provisional restoration. In most cases, by under-contouring or over-contouring the provision restoration, in specific areas, we can easily manipulate the gingival profile. This leads to thicker, more coronal gingival or apically placed gingival margins, respectively.
The following two clinical cases demonstrate how we can use the provisional restoration to achieve the ideal gingival profile.
Case 1
- A 31-year-old man is referred to the clinic because of a failing right maxillary central incisor.
- Clinical and radiographic examination shows a vertical root fracture.
- No active infections are present, and bone sounding confirms good buccal bone architecture.


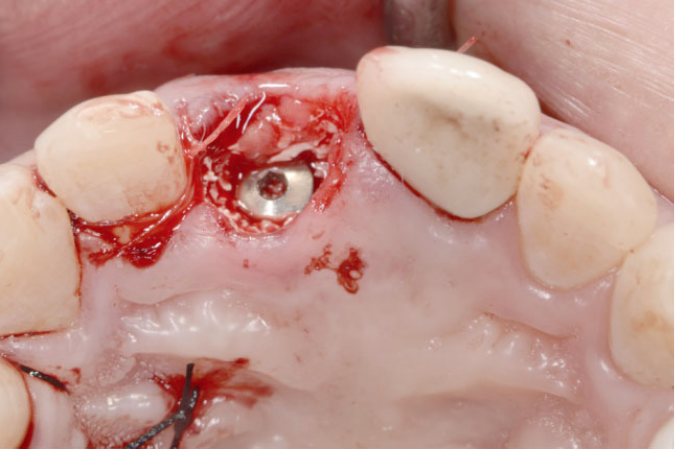
First, the right central incisor was extracted with minimal trauma. Intact buccal cortical plate was confirmed. Using a surgical sent, an Astra (Dentsply) 4.5×15 mm implant was placed, 3 mm below the free gingival margin. Bone graft (Endobon Zenograft Granules) was placed in the gap between the buccal plate and the implant fixture, along with a sub-epithelial connective graft placed in the gingival pouch.
Due to the stability of the implant and strength of the buccal plate, the implant was immediately restored with a non-functional screw-retained provisional. This was done using a putty index and bis-acrylic. This provisional was kept in place for 6 months.
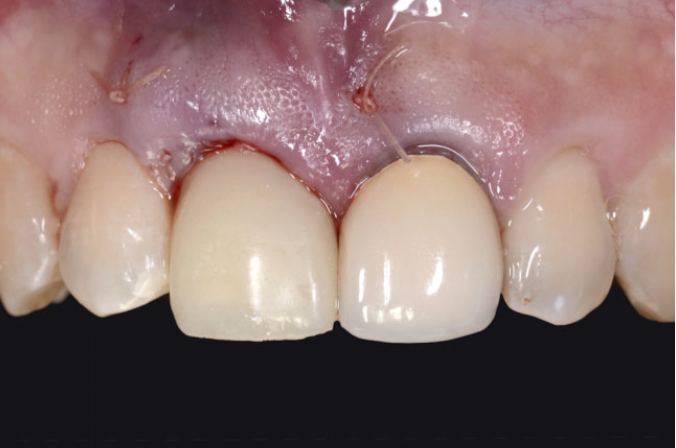
The only area of the gingiva that needed to be manipulated was the buccal gingival margin. Therefore, lower pressure was put on the buccal gingiva, by under contouring the provisional, resulting in the margin being seated more coronally. At the same time, more pressure was applied to the interproximals, by ideally contouring the provisionals, leading to fully supported interproximal papillae.
With the ideal gingival profile in place, the final restoration could now be made.


Case 2
- A 29-year-old female is referred to the clinic as she was unsatisfied with the implant crown placed on the upper right canine. She was specifically displeased with the gingival position surrounding the crown, as it was “lower” than her other canine.

Using a provisional restoration, more pressure applied to the buccal gingiva to ultimately position it more apically. The buccal margin of the provisional was gradually contoured by adding more restorative material (flowbale composite) over the course of 3 months.


Once the position of the buccal gingiva matched that of the left maxillary canine, the implant was permanently restored with a screw retained crown.
By creating select under-contoured areas in the provisional, we apply lower pressure to that area of the gingiva, and create a gingival margin located more coronal than original. By applying more pressure, by over-contouring the provisional in select areas, we can create more apically positioned gingival margins. After the pressure is applied, blanching is expected, but should disappear in 15 minutes. Restorative material can be added or subtracted depending on the tissue response. To get thicker peri-implant tissues, the final abutments should be concave. And all provisional should be highly polished to minimize plaque accumulation and to promote a health.
The cases presented were completed and reported by JUNG NAM, D.M.D., M.S., M.S.D., PRASIT ARANYARACHKUL, D.D.S., M.S.