
")
Class V lesions and root decays are very common. However, the durability of the restorations of these lesions is not promising. Once restored, we can expect a loss of retention, marginal excess, secondary caries and tissue inflammation. These problems are directly related to challenges in isolation, cervical fluid control, finishing and polishing. To solve these problems, a simple technique can be applied to both cervical and root caries, using a modified metal matrix method.
Cervical Lesions
A patient presents to your clinic with deep cervical class V lesions on the lower left first and second premolars. The full margins of the lesion cannot be seen as they are partially covered by the marginal gingiva. Challenges with isolation, moisture control and possible trauma to the tissues during polishing are evident.
Treatment using the modified matrix method
- First, local periapical infiltration with Lidocaine 2% with 1:100k epinephrine was done for patient’s comfort during the procedure.
- Rubber dental dam was placed.
- A standard universal Tofflemire metal matrix was tilted and pushed down adjacent to the tooth, and slid into the gingival sulcus. Once in the sulcus, the matrix was further pushed down to minimally displace the gingival tissue to gain full view of the lesion.
- The matrix was stabilized with wooden wedges on each side.
- Now with full view, safe application of the desired adhesive system and composite could be accomplished.
- Full polishing of the restoration can also be done, with the matrix in place.

Root Caries
In the case of root caries, the lack of enamel indicated the use of modified glass ionomer (RMGI). It has been shown in research that RMGIs bond better to root surfaces and increase durability of the final restoration, as compared to composite alone. However, when RMGI is used in bulk restorations, its polishing is challenging, leading to excessive finishing being necessary.
Treatment using the modified matrix method
- Local periapical infiltration with Lidocaine 2% with 1:100k epinephrine was done for patient comfort during the procedure.
- Rubber dental dam could not be placed, as it would obstruct the borders of the lesion.
- Ultrapack retraction cord #00 was placed on the facial surface of the lesion, and cavity preparation was completed using #2 carbide burs on a high-speed handpiece with copious water.
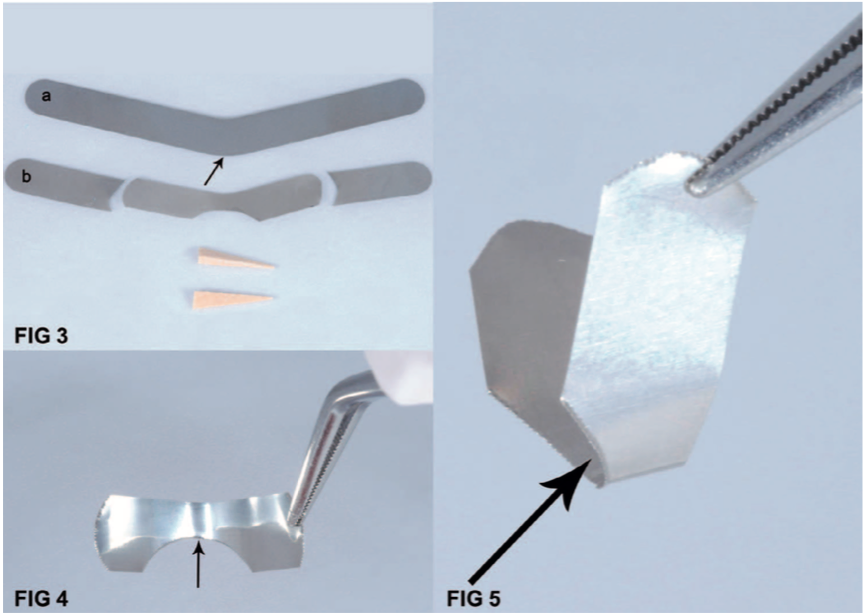
- A universal Tofflemire metal matrix was trimmed with scissors on its occlusal side to a width of 3mm (with a curvature opposite that of the band on that side), and the length was trimmed as needed for comfortable insertion. The trimmed occlusal portion of the matrix would now be the gingival side during insertion.
- The retraction cord was removed; the modified metal matrix was placed, gently pushed down into the gingival sulcus. The matrix was stabilized with wooden wedges on the mesial and distal sides.
- Now the RMGI with the correct shade was applied to the tooth. After complete setting, the modified matrix was removed.
- Complete polishing was done using fine diamond burs and medium/fine polishing discs.

This simple method of using materials already present in our offices can produce predictable and durable results. Due to the method’s slight displacement of the gingival tissue, isolation and smooth/ invisible margins can be achieved. This results in healthy tissues and an esthetic finish.
